China has tremendous resources, both human and financial, but it may now be facing a perfect storm of challenges. Its future is neither inevitable nor immutable, and its further evolution will be highly contingent on the content and efficacy of complex policy choices.
This is the core argument in a new volume,
Fateful Decisions: Choices that Will Shape China’s Future, edited by Shorenstein APARC Fellow
Thomas Fingar and China Program Director
Jean Oi. Forthcoming in May 2020 as part of Stanford University Press
monograph series with APARC, this volume combines the expertise of researchers from across the disciplines of sociology, history, economics, health policy, and political science, who examine the factors and constraints that are likely to determine how Chinese actors will manage the daunting challenges they now face.
One of these challenges — how China must soon achieve economic growth as it grapples with the realities of a rapidly aging population and a shrinking workforce — is the subject of a chapter authored by Karen Eggleston, the deputy director of APARC and director of the Center’s Asia Health Policy Program. In the following interview, Eggleston shares perspectives from her chapter, “Demographic Challenges.”
[To get more stories like this delivered to your inbox, sign up for our newsletters]
Q: What are some of the fateful decisions China is facing regarding the responsibilities of caring for a large, aging population?
A: China has achieved impressive improvements in health and longevity. It has implemented universal health coverage and is experimenting with financial support for long-term care for older adults. Yet significant gaps between the most- and least-privileged Chinese citizens persist, and in some cases are growing. As I have written elsewhere, it is not surprising that there are wide disparities in health and healthcare between different population subgroups in a country as populous, expansive, and diverse as China. How effectively and efficiently China meets these and other health- and aging-related issues will have a major impact on its ability to manage other social and economic challenges.
In the chapter I contributed to the volume Fateful Decisions, I note that China’s current population and demographic trends — including relatively rapid aging — reflect the success of earlier investments in infectious disease control, public health measures, and other contributors to mortality reduction. The lingering effects of family planning policies, historic preferences for sons, and rapid economic development are also major considerations. Together, these factors have produced a shrinking working-age population, a growing number of elderly, a gender imbalance, and hurdles for inclusive urbanization. An urgent question for China’s future is to what extent policies will ameliorate disparities in health, healthcare use, and the burden of medical spending.
The unfolding COVID-2019 outbreak is a powerful illustration of just how fateful decisions about health systems can be. Compared to the SARS outbreak almost two decades ago, China has been better prepared for this situation. SARS raised health system reform to the top of the political agenda and, many argue, played a direct role in China’s achieving universal health coverage and vastly strengthening the public health system.
But as China has become a middle-income global economic powerhouse in the years since SARS and the ensuing wave of health policy reforms, the expectations of its citizens about their health system have also risen. Has the health system, including public health and medical care, been strengthened to the same degree as other parts of the economy and public services? The impact of and lasting response to COVID-2019 may prove a litmus test.
Q: Why do these decisions about health carry such importance for China’s future development?
Through the last four decades, China has benefitted from a demographic dividend caused by the large bulge in the working-age population. But to achieve future economic growth and productivity, investments in human capital — particularly in health and education —need to be made. This higher productivity will, in turn, be the means by which a smaller workforce can support China’s large and growing cohort of retirees.
As we’ve already seen, health expenditures have increased rapidly as China has developed its system of universal health coverage. Double-digit health spending growth surpassed the rate of economic growth, and as a result, health spending absorbs an increasingly larger share of the total economy. China needs to make sure additional spending on health and elderly care is efficient and effective, while also addressing the nonmedical determinants of health and promoting healthy aging. The health system needs to be reengineered to emphasize prevention, provide coordinated health care for people with multiple chronic diseases, assure equitable access to rapidly changing medical technologies, and ensure long-term care for frail elderly, all without unsustainable increases in opportunity costs for China’s future generations.
Q: What is the Chinese government doing to improve healthcare quality and delivery, and what more could it do to affect meaningful change in its systems?
China’s current policies seek to balance individual responsibility, community support, and taxpayer redistribution through safety-net coverage funded by central and local governments. Like many countries, China would benefit from improved coordination across multiple agencies and structure incentives to avoid or mitigate unintended consequences that undermine the goals of its health system. Recent governance reforms, such as the creation of the National Healthcare Security Administration, aim to address these challenges.
China’s achievements and remaining challenges can be illustrated with the Healthcare Access and Quality Index (HAQ), which measures premature mortality from causes that should not occur if the individual had access to high-quality healthcare: among 195 countries and territories, China achieved the highest absolute increase in the HAQ Index from 2000 to 2016. However, the 43-point regional disparity in HAQ within China is the equivalent of the difference between Iceland (the highest HAQ in the world) and North Korea.
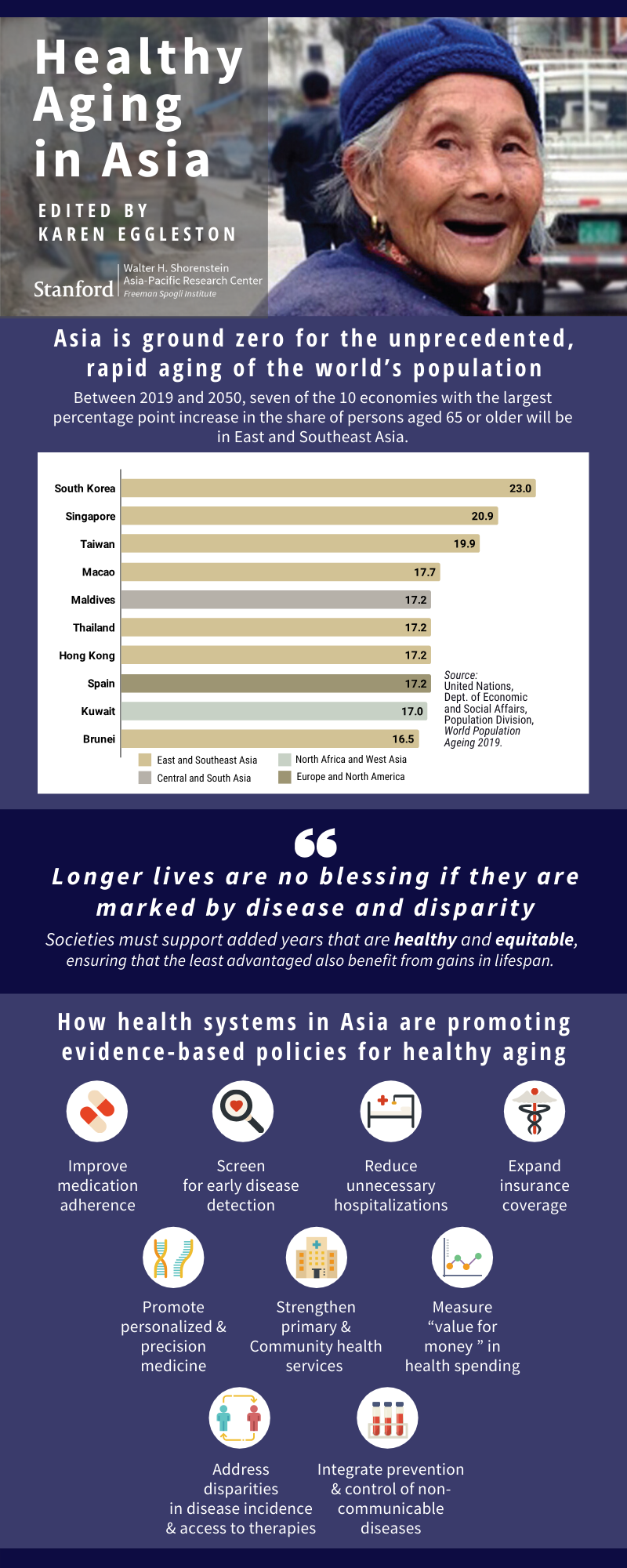
Q: The subject of your chapter, China’s demographic challenges, is one of the issues you investigate in your upcoming book, Healthy Aging in Asia. As you show in this volume, challenges at the intersection of aging, economics, demographic transition, and healthcare policy are not unique to China. How are other countries in Asia responding to them and what lessons could benefit China?
As I note in the introduction of Healthy Aging in Asia, the demographic transition from high to low fertility and mortality has been more rapid in much of Asia than in Europe and North America. That means social institutions, such as retirement, living arrangements, and intergenerational support, have to adapt quickly. For example, extending work-lives (as is happening in Japan) will be necessary but feasible only if the added years are healthy ones and equitable only if the least advantaged also benefit from healthy aging. The blessings of longevity dim when clouded by pain, disability, and loss of dignity.
Investment strategies in insurance and managing chronic conditions are also important considerations. Japan and Korea have adopted insurance systems for financing long-term care for frail elderly, while places like Hong Kong have good empirical research on chronic condition management.
No country or system has a “magic pill” to address these challenges, but the empirical evidence and rich policy experience documented in Healthy Aging from health systems as diverse as those in the cities of Singapore and Hong Kong to large economies such as Japan, India, and China can certainly be instructive.












 Karen Eggleston is a senior fellow at the Freeman Spogli Institute for International Studies (FSI) at Stanford University, director of the Stanford Asia Health Policy Program, and deputy director of the Walter H. Shorenstein Asia-Pacific Research Center at FSI. She is also a fellow with the Stanford Center for Innovation in Global Health and a faculty research fellow of the National Bureau of Economic Research (NBER). Eggleston earned her PhD in public policy from Harvard University, studied in China for two years, and was a Fulbright scholar in South Korea. Her research focuses on comparative health systems and health reform in Asia, especially China; government and market roles in the health sector; supply-side incentives; healthcare productivity; and economic aspects of demographic change.
Karen Eggleston is a senior fellow at the Freeman Spogli Institute for International Studies (FSI) at Stanford University, director of the Stanford Asia Health Policy Program, and deputy director of the Walter H. Shorenstein Asia-Pacific Research Center at FSI. She is also a fellow with the Stanford Center for Innovation in Global Health and a faculty research fellow of the National Bureau of Economic Research (NBER). Eggleston earned her PhD in public policy from Harvard University, studied in China for two years, and was a Fulbright scholar in South Korea. Her research focuses on comparative health systems and health reform in Asia, especially China; government and market roles in the health sector; supply-side incentives; healthcare productivity; and economic aspects of demographic change. Thomas Fingar is a Shorenstein Distinguished Fellow in the Shorenstein Asia-Pacific Research Center at Stanford University. From May 2005 through December 2008, he served as the first deputy director of national intelligence for analysis and, concurrently, as chairman of the National Intelligence Council. Previous positions include assistant secretary of state for Intelligence and Research (2000-2001, 2004–2005), principal deputy assistant secretary (2001–2003), deputy assistant secretary for analysis (1994–2000), director of the Office of Analysis for East Asia and the Pacific, and chief of the China Division. Fingar is a graduate of Cornell University (AB in government and history) and Stanford University (MA and PhD, both in political science). His most recent books are Uneasy Partnerships: China’s Engagement with Japan, the Koreas, and Russia in the Era of Reform (editor) (Stanford University Press, 2017); The New Great Game: China’s Relations with South and Central Asia in the Era of Reform (editor) (Stanford University Press, 2016); and Reducing Uncertainty: Intelligence Analysis and National Security (Stanford University Press, 2011).
Thomas Fingar is a Shorenstein Distinguished Fellow in the Shorenstein Asia-Pacific Research Center at Stanford University. From May 2005 through December 2008, he served as the first deputy director of national intelligence for analysis and, concurrently, as chairman of the National Intelligence Council. Previous positions include assistant secretary of state for Intelligence and Research (2000-2001, 2004–2005), principal deputy assistant secretary (2001–2003), deputy assistant secretary for analysis (1994–2000), director of the Office of Analysis for East Asia and the Pacific, and chief of the China Division. Fingar is a graduate of Cornell University (AB in government and history) and Stanford University (MA and PhD, both in political science). His most recent books are Uneasy Partnerships: China’s Engagement with Japan, the Koreas, and Russia in the Era of Reform (editor) (Stanford University Press, 2017); The New Great Game: China’s Relations with South and Central Asia in the Era of Reform (editor) (Stanford University Press, 2016); and Reducing Uncertainty: Intelligence Analysis and National Security (Stanford University Press, 2011).
 Jean C. Oi is the William Haas Professor of Chinese Politics in the Department of Political Science and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. She directs the China Program at the Walter H. Shorenstein Asia-Pacific Research Center and is the Lee Shau Kee Director of the Stanford Center at Peking University. Oi has published extensively on China’s reforms. Recent books include Zouping Revisited: Adaptive Governance in a Chinese County, coedited with Steven Goldstein (Stanford University Press, 2018), and Challenges in the Process of China’s Urbanization, coedited with Karen Eggleston and Yiming Wang (2017). Current research is on fiscal reform and local government debt, continuing SOE reforms, and the Belt and Road Initiative.
Jean C. Oi is the William Haas Professor of Chinese Politics in the Department of Political Science and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. She directs the China Program at the Walter H. Shorenstein Asia-Pacific Research Center and is the Lee Shau Kee Director of the Stanford Center at Peking University. Oi has published extensively on China’s reforms. Recent books include Zouping Revisited: Adaptive Governance in a Chinese County, coedited with Steven Goldstein (Stanford University Press, 2018), and Challenges in the Process of China’s Urbanization, coedited with Karen Eggleston and Yiming Wang (2017). Current research is on fiscal reform and local government debt, continuing SOE reforms, and the Belt and Road Initiative. Andrew G. Walder is the Denise O’Leary and Kent Thiry Professor of Sociology in the School of Humanities and Sciences, and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. A political sociologist, Walder has long specialized in the study of contemporary Chinese society and political economy. After receiving his PhD at the University of Michigan, he taught at Columbia, Harvard, and the Hong Kong University of Science and Technology. At Stanford he has served as chair of the Department of Sociology, director of the Asia-Pacific Research Center, and director of the Division of International, Comparative, and Area Studies in the School of Humanities and Sciences. His most recent books are Fractured Rebellion: The Beijing Red Guard Movement (2009), China under Mao: A Revolution Derailed (2015), and Agents of Disorder: Inside China’s Cultural Revolution (2019).
Andrew G. Walder is the Denise O’Leary and Kent Thiry Professor of Sociology in the School of Humanities and Sciences, and a senior fellow in the Freeman Spogli Institute for International Studies at Stanford University. A political sociologist, Walder has long specialized in the study of contemporary Chinese society and political economy. After receiving his PhD at the University of Michigan, he taught at Columbia, Harvard, and the Hong Kong University of Science and Technology. At Stanford he has served as chair of the Department of Sociology, director of the Asia-Pacific Research Center, and director of the Division of International, Comparative, and Area Studies in the School of Humanities and Sciences. His most recent books are Fractured Rebellion: The Beijing Red Guard Movement (2009), China under Mao: A Revolution Derailed (2015), and Agents of Disorder: Inside China’s Cultural Revolution (2019).









