


Call for papers: Conference on the economics of ageing
News Type
News
Date
Paragraphs
The Asia Health Policy Program at Stanford’s Shorenstein Asia-Pacific Research Center, in collaboration with scholars from Stanford Health Policy's Center on Demography and Economics of Health and Aging, the Stanford Institute for Economic Policy Research, and the Next World Program, is soliciting papers for the third annual workshop on the economics of ageing titled Financing Longevity: The Economics of Pensions, Health Insurance, Long-term Care and Disability Insurance held at Stanford from April 24-25, 2017, and for a related special issue of the Journal of the Economics of Ageing.
The triumph of longevity can pose a challenge to the fiscal integrity of public and private pension systems and other social support programs disproportionately used by older adults. High-income countries offer lessons – frequently cautionary tales – for low- and middle-income countries about how to design social protection programs to be sustainable in the face of population ageing. Technological change and income inequality interact with population ageing to threaten the sustainability and perceived fairness of conventional financing for many social programs. Promoting longer working lives and savings for retirement are obvious policy priorities; but in many cases the fiscal challenges are even more acute for other social programs, such as insurance systems for medical care, long-term care, and disability. Reform of entitlement programs is also often politically difficult, further highlighting how important it is for developing countries putting in place comprehensive social security systems to take account of the macroeconomic implications of population ageing.
The objective of the workshop is to explore the economics of ageing from the perspective of sustainable financing for longer lives. The workshop will bring together researchers to present recent empirical and theoretical research on the economics of ageing with special (yet not exclusive) foci on the following topics:
- Public and private roles in savings and retirement security
- Living and working in an Age of Longevity: Lessons for Finance
- Defined benefit, defined contribution, and innovations in design of pension programs
- Intergenerational and equity implications of different financing mechanisms for pensions and social insurance
- The impact of population aging on health insurance financing
- Economic incentives of long-term care insurance and disability insurance systems
- Precautionary savings and social protection system generosity
- Elderly cognitive function and financial planning
- Evaluation of policies aimed at increasing health and productivity of older adults
- Population ageing and financing economic growth
- Tax policies’ implications for capital deepening and investment in human capital
- The relationship between population age structure and capital market returns
- Evidence on policies designed to address disparities – gender, ethnic/racial, inter-regional, urban/rural – in old-age support
- The political economy of reforming pension systems as well as health, long-term care and disability insurance programs
Submission for the workshop
Interested authors are invited to submit a 1-page abstract by Sept. 30, 2016, to Karen Eggleston at karene@stanford.edu. The authors of accepted abstracts will be notified by Oct. 15, 2016, and completed draft papers will be expected by April 1, 2017.
Economy-class travel and accommodation costs for one author of each accepted paper will be covered by the organizers.
Invited authors are expected to submit their paper to the Journal of the Economics of Ageing. A selection of these papers will (assuming successful completion of the review process) be published in a special issue.
Submission to the special issue
Authors (also those interested who are not attending the workshop) are invited to submit papers for the special issue in the Journal of the Economics of Ageing by Aug. 1, 2017. Submissions should be made online. Please select article type “SI Financing Longevity.”
About the Next World Program
The Next World Program is a joint initiative of Harvard University’s Program on the Global Demography of Aging, the WDA Forum, Stanford’s Asia Health Policy Program, and Fudan University’s Working Group on Comparative Ageing Societies. These institutions organize an annual workshop and a special issue in the Journal of the Economics of Ageing on an important economic theme related to ageing societies.
More information can be found in the PDF below.
Hero Image

All News button
1
Xi'an summit explores China in transition
News Type
News
Date
Paragraphs
More than fifty experts met in Xi’an, China, for an international academic conference on demographic change and social development last week. Several scholars from the Freeman Spogli Institute for International Studies (FSI) spoke at the conference, including Karen Eggleston, Marcus Feldman, Jean Oi and Scott Rozelle.
The conference marked the 120th anniversary of Xi’an Jiaotong University’s founding and more than three decades of collaboration with Stanford scholars. Researchers at Xi’an Jiaotong University’s Institute for Population and Development Studies collaborate on policy-relevant research and educational activities with Stanford faculty at FSI as well as the Morrison Institute and Woods Institute.
For more information on FSI’s work in the areas of global health and medicine, please visit this page and the Asia Health Policy Program website.
Image

Hero Image
All News button
1
Rethinking illegal drug policy in Thailand
News Type
Q&As
Date
Paragraphs
In a Q&A, Stanford postdoctoral fellow Darika Saingam explains why Thailand's battle against drugs continues and what is needed to introduce good policy that works to prevent illegal drug trade and supports recovering addicts.
Despite Thailand’s decade-long crackdown on drugs, demand for illegal substances has risen. A green leaf drug known as ‘kratom’ is a symbol of this rise as young people eagerly adopt the drug for entertainment and join an older generation of laborers who chewed it to survive long hours of work in the fields—and are now heavily addicted. Curtailing substance abuse and its consequences takes good public policy and solutions must be area-specific and evidence-based, according to a Stanford postdoctoral fellow.
Darika Saingam, the 2015-16 Developing Asia Health Policy Postdoctoral Fellow, has conducted two cross-sectional surveys and more than 1,000 interviews with drug users, recovered addicts, and local public officials in an effort to better understand the evolution of substance abuse in southern Thailand.
At Stanford, she is preparing two papers that offer policy options suitable for Thailand and other developing countries in Southeast Asia. Saingam spoke with the Shorenstein Asia-Pacific Research Center (APARC) where she will give a public talk on May 17. The interview text below was edited for brevity.
For decades, Thailand has been an epicenter of drugs. Can you describe the extent of the problem today?
According to a 2014 report, 1.2 million people were involved in illegal drug activities across Thailand. The total number of drug cases saw a 41 percent increase from 2013 to 2014. New groups of drug traffickers are mobilizing while existing groups are still active. Drug users who are young become drug dealers as they get older. The number of drug users below 15 years of age has increased dramatically.
According to your research, what drives Thais toward illegal drug use and the trafficking business?
Adults in Thailand use drugs to relieve stress and counteract the effects of work. Adolescents use them for entertainment. Historically, farmers and laborers from rural areas of Thailand would use opium for pain relief. More recently, a consumable tablet known as yaba has become popular along with crystal methamphetamine and marijuana. Young people are increasingly using yaba and kratom.
Thailand is still a developing country, but it is industrializing quickly. Social and cultural norms have been shifting and people want an improved quality of life. A lot of young people are unemployed and lack social support and are therefore more likely to turn to drug trafficking for economic opportunity. The economic recession and political strife in countries bordering Thailand have exacerbated the situation.
Image

Image

Photos (left to right): A man holds up a kratom leaf. / Saingam examines kratom leaves as part of her research to understand illegal cultivation practices.
What is kratom and why is it popular?
For nearly a century, the native people of Thailand have chewed kratom. It is a leaf that grows on trees resembling a coffee plant. Historically, kratom was used to reduce strain following physical labor, to be able to work harder and longer, and to better tolerate heat and sunlight. Kratom is also embedded in Thai culture and given as a spiritual offering in religious ceremonies. My field research in the southern province of Nakhon Si Thammarat has shown that these motivations are still true today.
Within the past seven years, kratom use has skyrocketed and people are using it in increasingly harmful ways. Chewing kratom is not immediately harmful to health, but combining it with other substances is. This is the recent trend. Users have created new ways to consume it such as in a drink known as a ‘4x100.’ It contains boiled kratom leaves, cough syrup and soft drinks. Additional methamphetamines and benzodiazepines are sometimes added to that mixture.
What strategies must be employed to control substance abuse?
The first step is to realize that the patterns of substance abuse are specific to each location therefore solving the problem must also be. Drug usage is also dynamic. Placing hard control measures on one substance often provokes the emergence of another in its place therefore a holistic approach is important.
Thailand should employ multiple strategies toward effective prevention and control of substance abuse. These strategies include examining the problem and creating policies from an economic perspective (supply and demand), an institutional perspective (national and international drug control cooperation), and a social perspective (structural supports for recovered addicts and mobilization of public participation).
What is the Thai government doing to address the drug problem, and what could they be doing better?
Politicians in Thailand must do a better job at representing the people. Government health workers are often gathering information, assessing needs, and reporting findings to politicians, but these needs are not being accurately addressed. An example of this is politicians ordering to cut down kratom trees – a public display that does not get at the root cause of the problem. The reality is that drug users will quickly find substitutes. According to my study, of the regular users that stopped using kratom, more than 50 percent turned to alcohol instead and did so on a daily basis. This is merely a shift from one substance to another.
On the upside, a crop substitution program created under King Bhumibol Adulyadej offers a successful working model. The program works to replace opium poppy farming with cash crop production. It began in 1969 and is cited for helping an estimated 100,000 people convert their drug crop production to sustainable agricultural activities. Crops cultivated can be sold for profit in nearby towns. The program has also introduced a wide variety of crops and discouraged the slash-and-burn technique of clearing land. It is win-win because it stymies drug trade and provides economic opportunity while also being ecologically sound. This type of program should continue to be scaled up.
Can this model be co-opted elsewhere? What lessons from other countries could inform Thailand’s approach?
Yes, the model could plausibly be implemented in other areas in Thailand and in other Southeast Asian nations.
I think a judicial mechanism such as the kind seen in France could benefit the rural areas in Thailand. The French government has established centers across the country that act as branches of the court that try delinquency cases of minor to moderate severity, and also recommend support services for drug users. Members of the magistrate and civil society actors manage center operations thus placing some responsibility back onto the local community.
I believe an opportunity also exists for Thailand to legalize kratom. Legalization would show a respect for the cultural tradition of chewing kratom leaves and allow the government to suggest safer ways of using it. Bolivia has created a successful model of this through its legalization of coca leaves. Coca in its distilled form is cocaine, but left as a leaf, it is not a narcotic. Indigenous peoples are allowed to chew coca leaves. The government policy is being credited for a decrease in cocaine production as well.
Hero Image

All News button
1
Health economists press for chronic disease as top agenda item
News Type
News
Date
Paragraphs
Nearly 100 health economists from across the United States signed a pledge urging U.S. presidential candidates to make chronic disease a policy priority. Karen Eggleston, a scholar of comparative healthcare systems and director of Stanford’s Asia Health Policy Program, is one of the signatories.
The pledge calls upon the candidates to reset the national healthcare agenda to better address chronic disease, which causes seven out of 10 deaths in America and affects the economy through lost productivity and disability.
Read the pledge below.
Hero Image

All News button
1
Disparities in health and health care in Myanmar
Paragraphs
Myanmar (Burma) is undergoing a complex political and economic transformation, from a long civil war and military regime to a peace process and democratisation. Since 2011, the Myanmar Ministry of Health has started to rehabilitate the fragile health system, setting the goal of achieving universal health coverage by 2030. To achieve this target, Myanmar will have to face substantial challenges; arguably one of the most important difficulties is how to allocate limited health-care resources equitably and effectively.
All Publications button
1
Publication Date
Journal Publisher
The Lancet
Number
10008
The innovations in China’s primary health care reform: Development and characteristics of the community health services in Hangzhou
Paragraphs
Objective: This study focuses on Hangzhou, a Chinese city with a population of nine million urban and rural residents, to examine the successful development and innovation experience of its primary health care service system during the new health reform in China since 2009 and then disseminate the findings through international third parties.
Methods: Measures such as data analysis, study of documents and regulations, fieldwork, and expert discussions were used to systematically investigate primary health care in Hangzhou. The findings will have a profound practical impact on the health reform for nine million rural and urban residents throughout Hangzhou’s municipal boroughs.
Results: Community health services in Hangzhou are characterized as follows: They are government led; they are guaranteed with enough financing, personnel, facilities, and regulation; supported by the unified information platform; general practitioners have been assigned the key role of health ‘gatekeepers’; they provide primary care combined with basic public health services; there are integrated urban and rural health services and insurance coverage; and there is health care‐pension‐nursing integration and general practitioner ‐ contracted ‘smart’ services. Preliminary data collection and analysis indicate that the basic health status of Hangzhou residents is superior to that of residents of China as a whole, and some health indicators in Hangzhou are comparable to those in Western developed countries.
Conclusion: It is reasonable to believe that the primary health care level in China, including Hangzhou, will be further developed and promoted with indexed performance evaluations and more effective implementation of additional measures.
All Publications button
1
Publication Type
Journal Articles
Publication Date
Journal Publisher
Family Medicine and Community Health
In Myanmar, doctors protest "militarization" of healthcare
News Type
Commentary
Date
Paragraphs
Doctors, nurses and other medical staff in Myanmar are wearing black ribbons to protest the appointments of military personnel in the Ministry of Health.
“The Black Ribbon Movement Myanmar 2015,” which began on Facebook in early August, quickly amassed over 42,000 followers, and on Aug. 12, led the minister for health to drop plans to appoint military personnel to over 300 management positions within the ministry.
Writing for The Diplomat, Stanford visiting scholar Phyu Phyu Thin Zaw said the movement shows the dissatisfaction shared among her fellow doctors about the incursion of the military in the healthcare sector. She said it's also representative of greater injustices seen across Myanmar.
Four years have passed since the country transitioned from military rule toward democratization, and the Ministry of Health among other civic organizations still see the military exert influence over its operations.
Thin Zaw said she remains optimistic, though, and views the movement as a sign of the reemergence of a proactive civil society. The movement continues on this Facebook page.
The article published in The Diplomat can be found by clicking here.
Hero Image

All News button
1
Visiting fellow draws plan to scale up health index in China
News Type
News
Date
Paragraphs
China was for hundreds of years almost entirely an agricultural society, but modern industrialization changed that dynamic, and the impact on health has been startling.
Urbanization, population aging and changes in lifestyle (from mobile to sedentary) have led a transition from an acute to chronic disease-ridden society. Now, 10 percent of China’s adult population is diabetic or pre-diabetic—holding the number one place in the world.
Feng Lin and a team of researchers want to change that reality.
Lin is part of the Corporate Affiliates Program at the Shorenstein Asia-Pacific Research Center. A visiting fellow, Lin leads a research project focused on innovations in primary health care systems in China, a topic that is also the core of his work at ACON Biotechnology. Throughout his research, Lin has worked with health policy expert Karen Eggleston.
“Thirty to forty years ago, people were talking about infectious disease,” Lin says, referring to Chinese society. “Non-communicable diseases (NCDs) like diabetes didn’t even register. They were like the black sheep in the flock.”
Now, though, Lin says that China has reached a critical stage. NCDs have a noticeable presence, and the challenge for China is to create an effective healthcare system to serve its population of 1.3 billion. Its health delivery systems are not equipped to address and prevent diseases at such a high demand.
Lin believes that improving access to care by increasing the relevance of community health care centers, improving the quality of care and integrating IT infrastructure could provide pathways forward.
In pursuit of this, he is part of the team developing an open source health index with Yaping Du, a professor at Zhejiang University, and Randall Stafford, a professor of medicine at the Stanford Prevention Research Center.
The index is one of many activities that Lin is involved with at Stanford. Forging a new type of partnership with the Asia Health Policy Program, his company sponsored a public seminar series this past year.
Restructuring quality care
 Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Determining how to restructure China’s healthcare system is a tough challenge because it’s a bureaucratic hierarchy – multiple divisions traverse each province, prefecture, township and village.
In 2009, the Chinese government laid out aggressive reforms to its healthcare policy. Lin says he believes the most essential part of that plan is the empowerment of grassroots-level community healthcare centers.
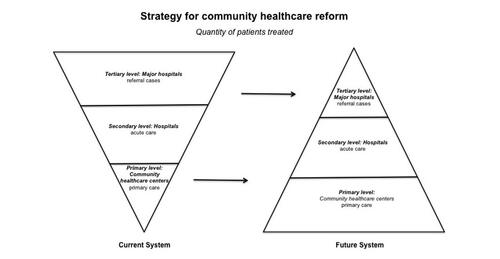
“You cannot just deal with primary level, you must look at the secondary and tertiary segments, too—a whole system approach,” he says.
Resembling a pyramid, China’s system has a finite number of top physicians who are mostly located at major hospitals. Patients who pursue services are likely to go to major hospitals in urban areas, instead of their local health community centers. About 90 percent of health care is delivered in hospitals—leading to overcrowding. Moreover, patients choose to self-treat or self-medicate which can lead to misdiagnosis.
Collecting data in Hangzhou, a coastal city just south of Shanghai (shown in map photo), Lin discovered that these trends could be explained by two reasons.
Patients have a low level of trust in community health centers, and local facilities lack capacity (e.g. having only 20 bed spaces) and expertise (e.g. employing medical personnel with sometimes outdated training). His analysis reinforced earlier outcomes found by Karen Eggleston.
Lin says the solution lies in increasing access to highly skilled physicians and organizing the system more efficiently.
Comparing China to the United States, Lin believes community healthcare centers should become main hubs for service delivery. The centers would operate as the first and last touchpoint for patient care, like “gatekeepers” in the U.S. system, administering advanced services and prevention programs like wellness education.
And while local centers are becoming more prevalent—China has more than 34,081 centers—development isn’t fast enough, not enough physicians exist, and patients aren’t actively choosing to redirect their services to community healthcare centers.
 Courtesy: Feng Lin
Courtesy: Feng Lin
Figure 1. Strategy for community healthcare center reform advocates "strength at the grassroots." Currently patients seek care at major hospitals as their first stop, but in the future system, patients will go primarily to grassroots community healthcare centers. Courtesy: Feng Lin
Creating ease
Chinese people are typically leery of the quality of health care available at community healthcare centers, and overcoming that trust deficit won’t be an easy task. However, Lin says it’s a matter of informing citizens about local services and training more physicians to deliver quality care.
To address quality concerns, the Chinese government has set out to expand medical training programs. Enhancing the expertise of current and future physicians in rural community healthcare centers is essential, Lin says.
The health index aims to empower patients so that they can determine the best medical accommodation available, and also create a mechanism that rewards good work.
The key is to create a participatory system, one that incentivizes the patient and the physician, he says.
Hosted digitally and in the public domain, the index will list all physicians throughout Zhejiang province. Patients and healthcare professionals can login and share their experience, providing a “satisfaction rating” of hospitals and community health care centers.
Beyond external contributions, the index will support data provided by China’s national Center for Disease Control and Prevention, and local centers for disease control, to include mortality rate and cause of death and many other indicators sourced from publicly available data.
“It will build up a kind of system that people can trust – something that people can rely on,” Lin says.
Similar platforms have been implemented in advanced industrialized nations. Lin hopes that the index will offer a model that could be applied nationwide.
“It’s nearly impossible to have a single policy apply,” he says. “But, if there’s a success in one area or a few areas, the central government will pick up that approach.”
Lin expects that his team will unveil the pilot program at a conference on general practice in October 2015. The conference aims to provide practical ways to improve primary care services and the education and training of general practitioners.
Map shown above is Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Hero Image

All News button
1
China provides universal health insurance at a fraction of the cost
News Type
Q&As
Date
Paragraphs
China’s demographic landscape is rapidly changing, and the government has responded by launching ambitious social and health service reforms to meet the changing needs of the country’s 1.3 billion people. This week, officials approved a five-year plan to develop a comprehensive nationwide social security network.
Karen Eggleston, the Asia Health Policy Program (AHPP) director and a Stanford Health Policy fellow, discusses the success of China’s health care reforms—including its recently established universal health care system—and the long road still ahead.
Why is the overall health and wellbeing of China’s population important globally?
There are many reasons why the health of China’s citizens matters within a larger global context. On the most basic level, China represents almost 20 percent of humanity. But it is also a major player in the world economy and it depends on having a healthy workforce, especially now that its population is aging more. The government’s ability to meet the needs of its underserved citizens contributes to a more productive and stable China, and works towards closing the huge gaps we see in human wellbeing across the world.
China also potentially offers a model for other developing countries, such as India, that may want to figure out how to make universal health coverage work at a tenth of the income of most of the countries that have put it into place before.
What are some of the biggest changes in China’s health care system since 1949?
One of the most significant changes is that China has achieved very basic universal health insurance coverage in a relatively short period of time.
Throughout the Mao period (1949–1978) there was a health care system linked to the centrally planned economy, which provided a basic level of coverage via government providers with a lot of regional variation. When economic reform came in 1980, large parts of the system—particularly financing for insurance—collapsed. The majority of China’s citizens were uninsured during the past few decades of very rapid social and economic development.
China’s overall population is changing quite dramatically, which means it has different health care needs, such as treating chronic disease and caring for an increasingly elderly population. The central government is trying to establish a system of accessible primary care—a concept that China’s barefoot doctors helped to pioneer but that fell into disarray—and health services that fit these new needs.
How does China’s basic health care system work? Are there segments of the population still not receiving adequate coverage and care?
China has had a system where people can select their own doctors. Patients usually want to go to clinics attached to the highest-reputation hospitals, but of course, when you are not insured you almost always by default go to where you can afford the care. “It is difficult to see the doctor, and it is expensive” has been the lament of patients in China, so an explicit goal of the health care reforms has been to address this.
The term “universal coverage” has different definitions. China initially put in place a form of insurance that only covers 20 or 30 percent of medical costs for the previously uninsured population, especially in rural areas. Benefits have expanded, but remain limited. As with the previous system, disparities in coverage still exist across the population. China not only has a huge population with huge economic differences, but within that there is a large migrant worker population. It is a challenge to figure out how to cover these citizens and how to provide them with access to better care. The government is quite aware there are segments of the population not receiving equal coverage, and it continues to strive to resolve the issue.
What are the greatest innovations in China’s health care system in recent years?
One of the most remarkable things China has achieved is really its new health insurance system. Even if the current coverage is not particularly generous it is nearly universal, and mechanisms are put in place each year to provide more generous coverage. China is also working on strengthening its primary care and population health services, infusing a huge sum of government money into these efforts. It is the only developing country of its per-capita income that has achieved such results so far.
Interestingly, a lot of people assume China achieved its universal coverage by mandate, while in fact the central government did so by subsidizing the cost for local governments and individuals. This reduces the burden, for example, on poorer rural governments and residents, and is one innovative way China is trying to eliminate the disparity in access to care.
Eggleston has recently published a working paper on China’s health care reforms since the Mao era on the AHPP website, as well as an article in the Milken Institute Review.
Gordon Liu, a Chinese government advisor on health care and the executive director of Peking University’s Health Economics and Management Institute, spoke at Stanford on May 29 on the future of China’s health care system.
Hero Image
All News button
1