Demographic change is fast becoming one of the most globally significant trends of the 21st century. Declining fertility rates and rising life expectancy -- two of the patterns triggering demographic change -- will cause vast socioeconomic strains, especially in the Asia-Pacific region, which has some of the world's most populous countries. Stanford health researcher Karen Eggleston says comparison and cross-collaboration are needed to induce creative solutions.
In an interview with the Office of International Affairs, Eggleston discusses her research approaches and partnerships in the study of healthcare systems and health policy in the Asia-Pacific region. She leads a multiyear research initative that examines comparative policy responses to demographic change in East Asia. Eggleston says the goal is to help move global health policy to a place where everyone has an "equal opportunity for a healthier and longer life."
Analyzing demographic change in China, Japan and South Korea is the focus of the book Aging Asia, an outcome of a conference between the Walter H. Shorenstein Asia-Pacific Research Center and the Stanford Center on Longevity.
Eggleston also coedited a special issue of the Journal of the Economics of Ageing with David Bloom, a professor at Harvard University, looking at a range of economic issues related to population change in China and India.
Hero Image
Karen Eggleston (left) confers with a healthcare worker at a primary care clinic in Hangzhou, China. | Robin Yao
For Matthew Kohrman and his students, the war against tobacco needs a new communications strategy.
After all, he noted, three times as many cigarettes are currently manufactured and sold worldwide than were in the 1960s. And the global cigarette industry is the greatest cause of preventable death on the planet today.
That’s why the Stanford associate professor of anthropology decided to teach an introductory seminar this spring, Anthro 182N, titled Smoke and Mirrors in Global Health. Kohrman led his 10 students on a journey into the “strange optics” that the global tobacco industry uses – and what to do about them.
As noted in the syllabus, “entrenched challenges” to global health require society to develop “new methods” to communicate the real truth about tobacco.
Just what are those “new methods?” At the culmination of the class, the students presented some variations on that theme. Their end-of-the-quarter projects were web-based efforts profiling various features of global tobacco. They included exposés on how academicians in China assist the industry in that country, humorous parodies and critiques of Philip Morris, and flawed approaches to tobacco control in South Korea.
They tackled big-picture questions, Kohrman said. For example, they asked what exactly constitutes cigarette manufacturing and how new strategies could help slow the spread of tobacco-related diseases worldwide.
Kohrman, the director of Stanford’s Cigarette Citadels project, envisioned his class as a way for students to offer some thought-provoking and original ideas grounded in solid data. After viewing the student projects, he was astounded – and proud.
“My overall impression has been a feeling of awe,” he said. “Mostly freshmen and sophomores, the students who enrolled in this new course quickly synthesized complex intellectual concepts introduced early in the quarter, conceived their own innovative project ideas, collected relevant data, generously worked with each other, designed apt strategies for evocatively visualizing their messages, and chose and implemented strong interactive media tools – most of which were utterly new to me.”
One of those students was Minkee Sohn, a communication major, who created a video, “Fresh Recruits,” to highlight what he believes is the hypocrisy in the language of some cigarette manufacturers’ recruitment efforts.
“While cigarette manufacturers,” Sohn said, “often frame smoking as an act of free choice, that choice is just an illusion. Free choice is denied to people in all stages of cigarette manufacturing and consumption.”
For example, he explained that children in the African country of Malawi are coerced to work with their families in tobacco fields. “It’s deeply disturbing to hear companies associate freedom with high-paying jobs in cigarette manufacturing.”
For biology major Annabel Chen, the most important thing she learned was to analyze information skeptically. “Industries like big tobacco have influences in unexpected places, so you always need to do sleuthing to find out the truth,” she said.
She chose to examine the links between tobacco and academic research in China. “Seeing as China is the biggest tobacco market in the world, this was a problem we needed to address.”
Kohrman appreciates how students like Sohn and Chen were willing to try an experimental course, never taught before, and which for many was outside of their comfort zone. He said the course will be taught again in 2015-16.
“Looking back, it was the perfect-size group for all the work and one-on-one teaching we did,” he said.
The course was a classic collaboration, according to Kohrman, who also credits Claudia Engel, a lecturer in the Anthropology Department who helped with the technology and his own experiences mentoring undergraduate research, all of which proved instrumental to designing Smoke and Mirrors in Global Health.
“It was a great success today,” he said after seeing the student projects on the last day of class. Tom Glynn, a top adviser to the American Cancer Society, was on hand to see the presentations.
Kohrman added, “Students got tremendous feedback, and there was lots of enthusiasm about how this experimental course unfolded.”
Clifton Parker is a writer for the Stanford News Service.
China was for hundreds of years almost entirely an agricultural society, but modern industrialization changed that dynamic, and the impact on health has been startling.
Urbanization, population aging and changes in lifestyle (from mobile to sedentary) have led a transition from an acute to chronic disease-ridden society. Now, 10 percent of China’s adult population is diabetic or pre-diabetic—holding the number one place in the world.
Feng Lin and a team of researchers want to change that reality.
Lin is part of the Corporate Affiliates Program at the Shorenstein Asia-Pacific Research Center. A visiting fellow, Lin leads a research project focused on innovations in primary health care systems in China, a topic that is also the core of his work at ACON Biotechnology. Throughout his research, Lin has worked with health policy expert Karen Eggleston.
“Thirty to forty years ago, people were talking about infectious disease,” Lin says, referring to Chinese society. “Non-communicable diseases (NCDs) like diabetes didn’t even register. They were like the black sheep in the flock.”
Now, though, Lin says that China has reached a critical stage. NCDs have a noticeable presence, and the challenge for China is to create an effective healthcare system to serve its population of 1.3 billion. Its health delivery systems are not equipped to address and prevent diseases at such a high demand.
Lin believes that improving access to care by increasing the relevance of community health care centers, improving the quality of care and integrating IT infrastructure could provide pathways forward.
In pursuit of this, he is part of the team developing an open source health index with Yaping Du, a professor at Zhejiang University, and Randall Stafford, a professor of medicine at the Stanford Prevention Research Center.
The index is one of many activities that Lin is involved with at Stanford. Forging a new type of partnership with the Asia Health Policy Program, his company sponsored a public seminar series this past year.
Determining how to restructure China’s healthcare system is a tough challenge because it’s a bureaucratic hierarchy – multiple divisions traverse each province, prefecture, township and village.
In 2009, the Chinese government laid out aggressive reforms to its healthcare policy. Lin says he believes the most essential part of that plan is the empowerment of grassroots-level community healthcare centers.
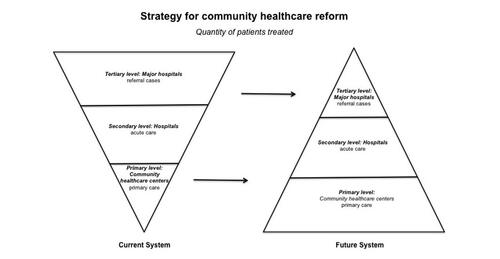
“You cannot just deal with primary level, you must look at the secondary and tertiary segments, too—a whole system approach,” he says.
Resembling a pyramid, China’s system has a finite number of top physicians who are mostly located at major hospitals. Patients who pursue services are likely to go to major hospitals in urban areas, instead of their local health community centers. About 90 percent of health care is delivered in hospitals—leading to overcrowding. Moreover, patients choose to self-treat or self-medicate which can lead to misdiagnosis.
Collecting data in Hangzhou, a coastal city just south of Shanghai (shown in map photo), Lin discovered that these trends could be explained by two reasons.
Patients have a low level of trust in community health centers, and local facilities lack capacity (e.g. having only 20 bed spaces) and expertise (e.g. employing medical personnel with sometimes outdated training). His analysis reinforced earlier outcomes found by Karen Eggleston.
Lin says the solution lies in increasing access to highly skilled physicians and organizing the system more efficiently.
Comparing China to the United States, Lin believes community healthcare centers should become main hubs for service delivery. The centers would operate as the first and last touchpoint for patient care, like “gatekeepers” in the U.S. system, administering advanced services and prevention programs like wellness education.
And while local centers are becoming more prevalent—China has more than 34,081 centers—development isn’t fast enough, not enough physicians exist, and patients aren’t actively choosing to redirect their services to community healthcare centers.
Courtesy: Feng Lin
Figure 1. Strategy for community healthcare center reform advocates "strength at the grassroots." Currently patients seek care at major hospitals as their first stop, but in the future system, patients will go primarily to grassroots community healthcare centers. Courtesy: Feng Lin
Creating ease
Chinese people are typically leery of the quality of health care available at community healthcare centers, and overcoming that trust deficit won’t be an easy task. However, Lin says it’s a matter of informing citizens about local services and training more physicians to deliver quality care.
To address quality concerns, the Chinese government has set out to expand medical training programs. Enhancing the expertise of current and future physicians in rural community healthcare centers is essential, Lin says.
The health index aims to empower patients so that they can determine the best medical accommodation available, and also create a mechanism that rewards good work.
The key is to create a participatory system, one that incentivizes the patient and the physician, he says.
Hosted digitally and in the public domain, the index will list all physicians throughout Zhejiang province. Patients and healthcare professionals can login and share their experience, providing a “satisfaction rating” of hospitals and community health care centers.
Beyond external contributions, the index will support data provided by China’s national Center for Disease Control and Prevention, and local centers for disease control, to include mortality rate and cause of death and many other indicators sourced from publicly available data.
“It will build up a kind of system that people can trust – something that people can rely on,” Lin says.
Similar platforms have been implemented in advanced industrialized nations. Lin hopes that the index will offer a model that could be applied nationwide.
“It’s nearly impossible to have a single policy apply,” he says. “But, if there’s a success in one area or a few areas, the central government will pick up that approach.”
Lin expects that his team will unveil the pilot program at a conference on general practice in October 2015. The conference aims to provide practical ways to improve primary care services and the education and training of general practitioners.
A rapidly aging population poses serious challenges for many countries around the world, particularly in Asia, home to the most populous countries. China and India account for nearly 36% of the world’s population, and are expected to face social and economic complications from demographic change in the next decades.
A special issue of the Journal of the Economics of Ageing explores these trends in a comparative perspective, “The Economic Implications of Population Ageing in China and India” (December 2014), co-edited by David Bloom, a professor at Harvard University’s School of Public Health, and Karen Eggleston, a Center Fellow at the Shorenstein Asia-Pacific Research Center.
“Population ageing represents uncharted waters for China and India,” Bloom and Eggleston write in their coauthored introduction.
The special issue is a collection of 10 articles that examine the economic benefits and potential dilemmas arising from decreased fertility and increased life expectancy, two trends that will impact the development and future trajectories of China and India at the micro- and macroeconomic levels.
Dropping or continued low birth rates imply fewer young people to refresh the labor market. But will this cause the workforce to shrink to an unsustainable level? Demand will increase for health care, long term care, and other social services that support the elderly. What must the government do to ensure adequate access to care?
Empirical data and commentary presented in the special issue seek to inform stakeholders about emerging patterns, and to provide insight on how to best address related policy challenges going forward.
“By adopting responsive behaviors and consultative institutions that address the challenges of population ageing in ways that are appropriate to their unique circumstances, China and India could reap the full economic and social benefits of longer, healthier lives,” they write.
The special issue includes an introduction by Bloom and Eggleston, a feature interview with Richard Suzman, and additional analysis by noted global health experts following each article. The titles and authors of the 10 original research articles are listed below:
Intergenerational co-residence and schooling (Anjini Kochar)
Regional disparities in adult height, educational attainment, and late-life cognition: Findings from the Longitudinal Aging Study in India (LASI) (Jinkook Lee, James P. Smith)
Healthy aging in China (James P. Smith, John Strauss, Yaohui Zhao)
Gender differences in cognition in China and reasons for change over time: Evidence from CHARLS (Xiaoyan Lei, James P. Smith, Xiaoting Sun, Yaohui Zhao)
Reprint of: Health outcomes and socio-economic status among the mid-aged and elderly in China: Evidence from the CHARLS national baseline data (Xiaoyan Lei, Xiaoting Sun, John Strauss, Yaohui Zhao, Gonghuan Yang, Perry Hu, Yisong Hu, Xiangjun Yin)
Should China introduce a social pension? (Bei Lu, Wenjiong He, John Piggott)
China’s age of abundance: When might it run out? (Yong Cai, Feng Wang, Ding Li, Xiwei Wu, Ke Shen)
The macroeconomic impact of non-communicable diseases in China and India: Estimates, projections, and comparisons (David E. Bloom, Elizabeth T. Cafiero-Fonseca, Mark E. McGovern, Klaus Prettner, Anderson Stanciole, Jonathan Weiss, Samuel Bakkila, Larry Rosenberg)
Economic development and gender inequality in cognition: A comparison of China and India, and of SAGE and the HRS sister studies (David Weir, Margaret Lay, Kenneth Langa)
Comparing the relationship between stature and later life health in six low and middle income countries (Mark E. McGovern)
The special issue of the Journal of the Economics of Ageing, vol. 4, pages 1-154 (December 2014) is available through Elsevier’s online platform ScienceDirect.
Hero Image
Asia health policy scholar Karen Eggleston (Center Right) learns about a digital health information system in a visit to a primary care center in Hangzhou, China in Oct. 2014. | Robin Yao
China and India account for nearly 36% of the world’s population. The two countries are expected to see an unprecedented, accelerated rate in elderly populations, a shift that has already begun and will continue in the years ahead as life expectancy continues to increase and fertility to decrease or remain below replacement levels. Examining demographic changes can offer a unique opportunity to enrich the theoretical and empirical understanding of the economic aspects of population ageing. This special issue of the Journal of the Economics of Ageing, coedited by David E. Bloom, the Clarence James Gamble Professor of Economics and Demography at Harvard University, and Karen Eggleston, a Center Fellow at the Shorenstein Asia-Pacific Research Center at Stanford University, is a diverse collection of micro- and macro-economic research on ageing in China and India. This introduction, co-written by Bloom and Eggleston, provides background context to demographic trends in China and India, connections between demographic and economic changes and possible behavioral and policy responses. The introduction also gives a preview of the main contributions of the 10 articles featured in the special issue, which cover topics such as the impact of non-communicable diseases in China and India, how parents’ expectations of co-residence with their children affects educational outcomes, and the prevention of cognitive decline in China.
China’s State Council has put forth draft legislation that would ban smoking in public spaces, part of the government’s larger advocacy efforts to help curb tobacco use nationwide. Matthew Kohrman, a professor of anthropology at Stanford University, said it’s a step forward but the ban’s long-term success would depend on local enforcement.
Despite popular belief, global cigarette production has tripled worldwide since the 1960s. Leading the surge has been China.
“China has become the world’s cigarette superpower,” said Kohrman, in an interview on National Public Radio’s program, Marketplace.
Moreover, local governments in China have become dependent on tax revenues generated from tobacco sales, thus reinforcing the cigarette’s ubiquity and ease of access.
China has implemented smoking bans in the past, but with varied success. Now rising healthcare costs caused by tobacco-related diseases are creating urgency for new regulations.
“Whether or not these new regulations will be enforced will, in the end, come down to local politics,” he said.
Matthew Kohrman is part of the Asia Health Policy Program at the Shorenstein Asia-Pacific Research Center, and leads the project, Cigarette Citadels, a peer-sourced mapping project that compiles more than 480 cigarette factories globally.
Economic and demographic transition pose major challenges for countries worldwide, particularly in large developing countries like China; however, strengthening social welfare programs can offset negative effects and help promote a sustainable future, according to Karen Eggleston, a scholar of Asia health policy at Stanford University.
“Unprecedented economic growth in China spanning the last three decades has lifted hundreds of millions out of poverty and restored China to the prominence in the world economy that it once enjoyed centuries ago,” said Eggleston, who is a Center Fellow at the Walter H. Shorenstein Asia-Pacific Research Center.
“Demographic change not only shapes the trajectory of [its] development, but interacts with macroeconomic and microeconomic forces” in numerous ways.
Eggleston, who presented “China’s Demographic Change in Comparative Perspective: Implications for Labor Markets and Sustainable Development” at the Jackson Hole 2014 Economic Symposium “Re-evaluating Labor Market Dynamics,” says a combination of societal changes makes China distinctive, and that the country can offer insights in comparative perspective. She joined two other experts for a panel discussion on demographics during the three-day conference led by the Federal Reserve Bank of Kansas City, which draws dozens of central bankers, policymakers, academics, and economists from around the world.
The research stems from a project that Eggleston heads on policy responses to demographic change in Asia. The initiative, which is a part of the Asia Health Policy Program, grew out of a 2009 conference cosponsored by the Global Aging Program at the Stanford Center on Longevity. Its outcomes have included the publication, Aging Asia, a special issue of the Journal of the Economics of Aging focused on China and India co-edited with David Bloom of Harvard University, and two forthcoming books on urbanization and demographic change in Asia.
China in flux
China is the most populous country in the world with more than 1.3 billion people. Its sheer size alone creates heavy demands as demographics change, and the economy continues its shift from a centrally-planned system to a market-based system.
China’s population age 60 and older is projected to increase from one-tenth of the population in year 2000 to a staggering one-third by year 2060. Simultaneously, the population age 14 and under is projected to decrease by one-third between years 2010 and 2055 (Figure 2).
Eggleston, and others who closely watch the situation, say these demographic changes will bring a myriad of challenges to the labor market and to cultural norms related to intergenerational support, work and retirement.
China’s low birth rates have largely been influenced by family planning campaigns that begun in the early 1970s, and later, the “one child policy,” a population control policy that allowed for the birth of only a single child in many families. Recently, the government has relaxed that policy, and analysts believe the change will eventually help to balance the population age structure and infuse the workforce with new employees, filling the void caused by retiring workers in the coming years.
In the meantime, preparing support structures for the older generations’ departure from the labor market is essential. Social welfare programs, including health insurance and retirement and childcare services, will see significant demand, and require restructuring to handle the influx.
China’s aging population experience is similar to other countries in Asia. Japan, South Korea and India are also projected to see significant increase in median age over the next 30 years (Figure 1).
Eggleston says China has made positive steps toward restructuring its institutions, including establishing government-subsidized health insurance programs and reforming pension systems. Most notably since 2002, China took a large step towards universal health care by implementing the New Rural Cooperative Medical Scheme for rural residents. Now, nearly all citizens have access to basic medical care, which can support healthy aging as well as mitigate large “precautionary savings” and help those struck by medical conditions requiring significant services.
A pension system for people in China’s rural areas, developed by the government in 2009, also set up a supportive system by providing increased transfers for seniors, and, interestingly, supporting labor markets by easing the worries of adult children who migrate to urban areas for work.
China has been forward thinking with its related public policies, but it certainly can do more, Eggleston says. Integrating technology into its health systems, and making its services more fiscally responsible could improve efficiency, and expand access to care.
Shorenstein APARC616 Serra StreetEncina Hall E301Stanford, CA 94305-6055
(650) 725-2507
(650) 723-6530
0
minhpham@stanford.edu
pham_ngoc_minh.jpg
Ph.D.
Pham Ngoc Minh joins the Walter H. Shorenstein Asia-Pacific Research Center (Shorenstein APARC) as the 2014-2015 Developing Asia Health Policy Fellow as a health researcher and administrator.
His main interests are public health, disease prevention and the rural-urban divide in developing countries. At Stanford, Pham will be studying epidemiological trends and policy perspectives of diabetes in Vietnam, particularly those among adults in mountainous areas of that country. Pham has more than six years of experience working as a medical lecturer at the Thai Nguyen University of Medicine and Pharmacy in Vietnam, and spent two and a half years conducting postdoctoral research in Japan. He received a Bachelor of Medicine from the Thai Nguyen University of Medicine and Pharmacy, a BA in English from Hanoi University, an MPH from the University of Melbourne, and a PhD in medical science from Kyushu University.
2014-2015 Developing Asia Health Policy Postdoctoral Fellow
On April 3, 2014, Karen Eggleston provided testimony before the U.S-China Economic and Security Review Commission at the "Hearing on China’s Healthcare Sector, Drug Safety, and the U.S.-China Trade in Medical Products."
Some of the questions addressed included:
How has the nature of disease in China changed in recent decades? What kind of burden might it place on China's future development?
If providers are "inducing" demand by overprescribing drugs, it this a public health crisis in the making?
Can you outline the pros and cons of market reform in China's healthcare sector? What might be the proper role of the state of improving healthcare delivery?
Kan bing nan, kan bing gui (inaccessible and unaffordable healthcare) is one of the top concerns of ordinary Chinese. Which groups are most affected? Is this a global problem, what lessons can we learn from China?
The pharmaceuticals industry features in China's Medium and Long-term Plan for Science and Technology (2006-2020), as well as in more recent measures to promote indigenous innovation and industrial upgrading. Is it fair to say that the Chinese government is prioritizing domestic pharmaceutical companies, which foster economic growth, over the welfare of patients?
What were major successes and failures of the 2009 healthcare reforms [in China]? How have those reforms been supplemented by more recent measures (e.g. last November's Third Plenum)?
What aspects of China's healthcare reform should the U.S. government and U.S. companies pay most attention to?
We use retrospectively reported data on smoking behavior of residents of Mainland China and Taiwan to compare and contrast patterns in smoking behavior over the life-course of individuals in these two regions. Because we construct the life-history of smoking for all survey respondents, our data cover an exceptionally long period of time – up to fifty years in both samples. During this period, both societies experienced substantial social and economic changes. The two regions developed at much different rates and the political systems of the two areas evolved in very different ways. More importantly, governments in the two areas set policies that caused the flow of information about the health risks of smoking to differ across the regions and over time. We exploit these differences, using counts of articles in newspapers from 1951 to present, to explore whether and how the arrival of information affected life-course smoking decisions of residents in the two areas. We also present evidence that suggests how prices/taxes and key historical events might have affected decisions to smoke.
Dean Lillard received his PhD in economics from the University of Chicago in 1991. From 1991 to 2012, he was a faculty member and senior research associate in the Department of Policy Analysis and Management at Cornell University. In August 2012 he joined the Department Human Sciences at Ohio State University as an Associate Professor. He is Director and Project Manager of the Cross-National Equivalent File study that produces cross-national data. He is a member of the American Economics Association, the Population Association of America, the International Association for Research on Income and Wealth, the International Health Economics Association, the American Society for Health Economics, a Research Associate at the German Institute for Economic Research in Berlin, Germany, and a Research Associate of the National Bureau of Economic Research. He serves on the advisory board of the Danish National Institute for Social Research in Copenhagen, Denmark and the Cross-National Studies: Interdisciplinary Research and Training Program – a collaborative program run by the Polish Academy of Sciences (PAN), and together with the Mershon Centre at OSU.
Dean Lillard's current research focuses on health economics, the economics of schooling, and international comparisons of economic behavior. His research in health economics is primarily focused on the economics of the marketing and consumption of cigarettes and alcohol. His research on the economics of schooling includes studies of direct effects of policy on educational outcomes and on the role that education plays in other economic behaviors such as smoking, production of health, and earnings. His cross-national research ranges widely from comparisons of the role that obesity plays in determining labor market outcomes to comparisons of smoking behavior cross-nationally.



 Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
Hangzhou, Zhejiang Province, China. Photo credit: Wikimedia Commons
 Courtesy: Feng Lin
Courtesy: Feng Lin





